Different Strokes
It's good to know the typical symptoms, but strokes can happen without them
I had a stroke last May, after a series of "warning strokes" over the previous three months. Its symptoms were so unusual that I didn't get a firm diagnosis of "stroke" until two months later. I haven't recovered, as people often do; most of the symptoms are still with me, but I've learned to live with them: a slight numbness in my right chest and upper lip, with paresthesia- the pins-and-needles feeling- in my right hand and forearm. I call it my mojo hand.

Some classic stroke symptoms I never had.
Zaandam image courtesy of Wikipedia commons.
The first warning came after my wife and I had worked out at the YMCA. She had run into Aldi for a quick purchase and I was waiting in the car. Suddenly I had a sinking feeling- that's the only way I can describe it, though I didn't fall over or pass out. Floaters started to appear in the right side of my field of vision, and my right hand felt numb.
When Kae came back I told her she had better drive because I wasn't feeling well and wasn't sure what was going on. We went home and got on the phone to consult our nurse practitioner daughter, Robin. "Get to the hospital" was the bottom line. A big one, she said, not a walk-in clinic but one with facilities to do the full stroke protocol. So we headed for the nearest big hospital, Wuesthoff, in Rockledge.
I wasn't a typical candidate for stroke. I wasn't overweight. I drank in moderation and didn't smoke. I did weight workouts, kayaked, bicycled and took long walks. Every week or two I played a slow game of tennis with Kae. A couple years before, I had had a full "nuclear" stress test, running and gasping on a treadmill, which confirmed I had no significant blockages. The cardiologist said I could expect ten-plus years of active life ahead.
The stroke protocol starts with an IV being inserted in your arm. Then you get wheeled to various parts of the hospital for CT scans, MRIs, more tests than you've ever heard of. After a few hours of this, I was released with a diagnosis of a probable "transient ischemic attack" (TIA), sometimes described as a "warning stroke".
Within a couple of days, the "TIAs" were back again, this time including the right leg. On Robin's advice, I went to a hospital further away, Holmes Regional, which had a stroke center. They would be able to administer the "clot buster" drug to dissolve a clot, if necessary. This time it was an overnight stay.
After a few hours in the hospital I began to feel guilty. Here I was relaxing in bed, reading and surfing the net, feeling fine (in between tests), while all around me were people in pain who really needed all this care. I never asked a nurse for anything except coffee. When they forgot, I didn't buzz.
The staff neurologist said, among other remarks, that he doubted that it was a stroke. He suspected a pinched nerve along the spine might have caused most of the symptoms. But there was also a suspicion I might be having atrial fibrillation- an irregular, rapid heatbeat- so I was fitted with a heart monitor to wear for the next month.
They sent me home with a prescription for a higher dose of statin and a full strength aspirin daily- both already started in the hospital. I made an appointment for followup with a neurologist near home.
The test reports all confirmed no significant blockages or narrowing of blood vessels. But they brought a litany of bad news, not all related to my symptoms: Shrinkage of the brain, normal for my age but not welcome news. Evidence of emphysema in the lungs- I was never troubled with shortness of breath, but maybe I would be. And "spinal deterioration", under several Latin terms denoting narrowing of nerve passages, which could potentially compress nerves; lots of arthritis, up and down the spine. A slipped disk in the lumbar region, which had flared up a few years back but didn't trouble me much anymore.
As for spinal deterioration, Robin said "I could have told that by looking at you." Kae had been telling me to stand up straight for years. I did try, but often didn't remember. I had tried an electronic device that warned you of slumping, but you had to bend way over to trigger it. Also tried a sort of harness that forced me to hold my shoulders back, but it didn't seem to help.
When I saw my neurologist, she put me through a series of hand, arm and leg movements that were becoming familiar, and saw no problems. Was there any help for the spinal problems and arthritis? No, just continuing to exercise. She warned against movements that extend the spine. Asked for clarification she said "no bungee jumping." That was a restriction I could live with. She said I should cut my drinking to no more than one a day. Which I did, for awhile.
I completed a month of heart monitoring and mailed the device back. Getting the results was a struggle. When I phoned the cardiologist who "read" the monitor data, his receptionist said he couldn't give me the results, he was just the reader; I needed to contact the doctor who had ordered the monitor. This was a hospital staff cardiologist. When I managed to contact him by phone, he said I should have the results sent to my neurologist. So I did.
When I called my neurologist's office to ask about the results, I was told she couldn't give me the results, that I needed to see my cardiologist. After a bit of argument, the office administrator came on the line and repeated forcefully that I had to have a cardiologist give me the test results. OK- could they refer me to a cardiologist? Oh yes, there was one nearby; they'd write up a referral package right away and I could pick it up that morning. Could they also give me a copy of the heart monitor report? Sure.
I may have been a little deceptive here- I didn't tell them I could read. The report said in fairly plain English that there was no atrial fibrillation, nor any of the other patterns they checked for. I asked Robin to read it; she confirmed there was no significant problem- only one minor irregularity in the heartbeat that she said was not a concern. (She had worked for years in her specialty of cardiology.) So I saved myself and Medicare a few bucks by not seeing that cardiologist.
In April I had another episode of symptoms, but again they went away after a few minutes, and I didn't choose to go back to the hospital.
One morning in May, during my weight workout at the gym, I started to feel dizzy. I stopped and headed toward a chair to rest, but started feeling numb in my right hand. I told one of the trainers I might be having a mini-stroke (TIA) and asked if she had any aspirin. She found me a packet of some compound that included aspirin.
I had decided to go to the hospital, but waited a few minutes for Kae to finish her yoga class. As I sat resting, a young woman sat down beside me, waiting for the zumba class to start. She asked if I was feeling OK, and I told her what was going on.
"Would you like me to pray with you?" she asked. I held her hand for a minute while she prayed. Which was very thoughtful of her, and might have helped.
When Kae came out, we went straight to Holmes, where I was admitted. It was hard getting the IV in this time, since the same site had been mined repeatedly. I cautioned them that I shouldn't be given the clot buster drug, as I had taken Cialis the night before (It stays in your system for three days.)
(I don't know whether the clot-buster could have helped at that point; one neurologist told me later that it wouldn't be indicated with symptoms as mild as mine.)
Same old routine in the hospital: relaxing, feeling fine, under observation, with people in genuine need all around me. In the morning my neurologist came by, put me through the usual examination and seemed to find nothing new. She remarked that "sometimes these things come and go, and sometimes they come to stay." After she left, the numbness came back, but subsided after a few minutes. I probably could have stayed, but was set on going home.
After my release, Kae and I ran some errands, stopping at different stores. While I was waiting in the car for her at one store, the numbness came back. It subsided, then came back again after we returned home. This time it stayed.
At first, I was determined not to go back to the hospital. What would they do, after all, but stick in another IV and keep me under observation. I was pretty sure what Robin would advise, so I didn't call to ask.
But after a few hours I began to wonder. I called my neurologist, who as usual was not available; then called my GP's office. Asking various receptionists and nurses if I should go back to the hospital, I got noncommital answers, including: "I don't know, but if you think you should be admitted, you should certainly get admitted."
I stayed home, but continued bugging doctors' offices- wasn't there some treatment for this? Finally my neurologist scheduled some nerve testing for the following week, including a nerve conduction study.
Nerve testing lasted most of the following Friday morning, followed by an MRI of the lower spine. There was significant weakness in the nerve signals in the right arm and leg, suggestive of pinched nerves, and suggesting "a significant component of carpal tunnel syndrome."
For the second time, my neurologist suggested that I seek a second opinion from an out-of-town clinic specializing in neurology; there were several she recommended. She was still vague about her diagnosis, and somewhat apologetic. "Lots of people have weird feelings in their arms and legs, that we can't definitely explain."
I don't know if it was unique to this clinic, but referrals seemed to be a big challenge. They would send a referral to clinic X; I would call X after a few days and hear that it was not received. Sometimes it was the wrong fax number or the wrong department; sometimes I'd have definite confirmation that my clinic had sent it and definite confirmation from X that they had not received it.
Finally I looked up one of the clinics on the internet and requested an appointment, via their web portal, with a neurologist who was highly rated by patients. A few weeks later I made a three hour drive to the clinic with a bundle of test reports in hand.
Naturally, I had made an appointment with the wrong doctor. "I'm a surgeon," he explained. "You need to see a good diagnostician, like Dr. A." They were all listed as neurologists on the website; who would know? But I did get some more information.
First, the written reports were no use- he needed to see the actual digital records from the MRI's, CT scans etc. Also, I asked about the spinal deterioration- was there anything I could do to slow the progress of the arthritis and associated spinal problems?
"Oh," he said, grinning, "You want to turn back the hands of time. Can't be done." It was just normal ageing and there was no help for it.
So I made my appointment with Dr. A for the next available time, a few weeks later, and set about collecting my medical records. Which was very easy; all the digital records were available in CD or DVD form, with the supporting reports on paper. I had copies sent to Dr. A and also collected my own set. The hospitals and clinics made no fuss about this, and there was not even a charge, except in one case for a blank CD.
Meanwhile, I searched the internet for exercises or other therapy related to my several spinal conditions. Several references discussed the McKenzie method, a system of physical therapy developed by a New Zealand physical therapist and used in many clinics, though none nearby. I also found a list of exercises published by the Florida Hospital Spine Center. It may not have been intended for public distribution, since I found no link to it on any of their web pages, but the page itself appeared in my search.
I started doing some of these exercises daily, after clearing some of them with my neurologist (they involved extensions.) She advised doing the movements slowly.
After a few weeks and another long drive, I was back at the clinic to see Dr. A. Had they received all my records? Yes, but they couldn't read in the MRI results. Nor could they read them from my CDs- into the archiving system, at least. Luckily, the doctor could display them via other software on his computer.
So I told Dr. A's nurse, and then Dr. A, the entire narrative above. My main question was whether he could provide a better diagnosis. "What do you think of all this?" he asked. Which caught me flat-footed- I had never actually tried to reason out a diagnosis. Instead I clung to the indications that I hadn't had a stroke but some problems with the spine instead, which seemed better somehow. No spinal condition would have caused the floaters or the lip numbness, and all the symptoms had come at the same time.
"You had a stroke," he said. "A little one. I don't like the term mini-stroke." But I was not at risk for a major stroke. He approved my statin dosage, but cut the aspirin to one low-dose pill a day because I'd had trouble with gastric reflux.
He recommended regular exercise, both aerobic and weight-bearing. He emphasized that the biggest risk factor for stroke was age. "They won't tell you that, because they can't do anything about it."
I showed him the list of exercises I was doing and asked if they would help. "You can do these exercises if you have pain," he said; otherwise there was no point.
He asked specifics about my drinking, and reiterated the standard definition of "moderate" for men my age, which I had heard and read before but perhaps never fully taken in: two 12 ounce beers a day, or two 5 ounce glasses of wine, or one 1.5 ounce shot of 80 proof liquor. I realized my former "moderate" alcohol intake was higher, maybe 50% more, but didn't discuss this with him.
"But if it's only that much," he said, referring to the official moderate level, "if that's your limit, then you're OK. In fact, it's beneficial."
"Then you don't think it's a statistical artifact?" I said, referring to the occasional news about the "healthy effects" of red wine drinking.
Much as I enjoyed my booze, I always took these reports with a grain of salt. There's reservatrol in the wine, sure, but you can get that from pasteurized grape juice or pills. Back in grad school, we considered that if you found a correlation but couldn't explain the physical mechanism that caused it, all you had was an interesting correlation- no proof of a relationship, not even much in the way of evidence.
Dr. A then asked a remarkable question- remarkable in that my other doctors never asked it: "Have you seen a hand specialist about the carpal tunnel symptom?"
In his notes he said the symptoms in my hand might go away, or might be permanent. I could seek treatment but it would only be palliative, not a cure.
Back home again, I calibrated our wine glasses for a five ounce pour, and made an appointment with an orthopedic hand specialist in another distant but well-regarded clinic.
This specialist looked over the nerve conduction results and did some examination of his own. He was skeptical of the carpal tunnel diagnosis, first because my symptoms affected all five fingers, not all of which were connected to the nerve running though the carpal tunnel. Also because it would have been odd for carpal tunnel to flare up just at the same time as the arm and leg numbness and the floaters.
For the "acid test", he injected a steroid into the nerve just above the wrist. "If you don't see improvement soon, then I'd say it's not carpal tunnel, but something higher up." (i.e. the spine or the brain.)
He also suggested I see an upper spine specialist. "Neurologists are great for diagnosing these symptoms," he said, "But when you ask what to do about it, they don't have much to offer."
The hand symptoms never improved. I was back a month later to see an upper spine specialist.
"Is it possible to slow the spinal deterioration and arthritis?" I asked. "We can slow it, and we can stop it," he replied.
"Have you seen those old guys in the supermarket, leaning over the shopping cart to support themselves? They can move their legs OK, but they don't know where their feet are."
He wrote out a prescription for physical therapy for "spinal stabilization", which he said any certified physical therapist would know how to do. If my symptoms didn't improve after three months, I was to see him again. In retrospect, I'm not sure if he meant the hand symptoms or the spinal deterioration.
I went to a physical therapy clinic and signed up with a therapist named Warren, who had treated Kae some years back and who she highly recommended. He turned out to be an avid bicyclist, so we had a bit to talk about. I told him about several good trails he hadn't tried.
Each session began with five minutes on a "hand bike". Then there were exercises, similar to Florida Hospital's list. Finally, there was a neck massage, followed by an ice pack for ten minutes or so.
During the first weeks of therapy, I could notice my posture improving. Sometimes I would catch myself slumping, and it didn't feel right- I'd square my shoulders right away. When I visited my daughter Patti, she noticed the difference. "You used to walk like a gorilla," she said.
Warren doubted that therapy could stop spinal deterioration, but agreed it could be slowed. I remarked that I was must be unusual in seeking out physical therapy when not actually in pain. He agreed, but said "If you wait until you feel pain, it will be that much worse."
After three weeks, Warren said he noticed a big change in my neck; it had been quite stiff before but now was looser. After a month of therapy, I was released, assigned to keep up the exercises daily at home. Not a full session, but 15-20 minutes using a few of the dozen or so exercises- "pick and choose," Warren said.
I was scheduled for a followup appointment with my neurologist, but decided to go with a different one. Most of those I called were not accepting new patients, but I was finally booked with one in a nearby clinic.
When I saw her, she concurred with Dr. A's diagnosis and my current meds, but told me I should avoid alcohol entirely. When I protested that my usage was moderate, she said maybe one drink a day would be OK. She also told me there was a risk of stroke with any of the Viagra-like meds.
Now I had three different neurologists' recommendations for alcohol exposure: 0, 1 or 2 drinks per day. A conservative approach would have been to go with the lowest exposure, or at least the average. But I preferred Dr. A's recommendation.
Within a few weeks, I was notified that my neurologist was leaving the local clinic for a new job out of town. I was assured that a qualified neurologist would be there to cover my next appointment, but they didn't know who.
As the New Year approached, I was resigned to a permanent mojo hand. I would see the upper spine specialist again, but doubted he would be able to help. The symptoms were not debilitating, just an annoyance that I was learning to ignore.
I still had normal strength and mobility in the right hand, and the normal senses of touch and of hot and cold. But the pins-snd-needles feeling distorted my tactile perception. If I had a metal object in my right pocket along with my car keys, it was hard to tell which was which, and I might drop the object when bringing out my keys, without realizing it.
My typing is slower. At first I had to concentrate on the right hand keys, and had a terrible time finding the period. But perhaps because I had been typing for sixty-odd years, I was able to re-learn to an extent.
For most complex movements of the right hand, I had to look at the hand to be sure what I was doing. I had been trying to learn piano, and gave up the effort. The right hand plays the melody, usually pressng a different key on every beat, and with the paresthesia it was just too aggravating to make those movements accurately and on time. (No backspace key, either.)
The question of drinking still bothered me. I could keep to the strict limit of two beers or two glasses of wine a night, but skipping them for a day was hard- I almost never did. I was technically "moderate", but still worried that daily drinking was not good even at that level.
Somewhere online I saw a reference to Dry January, a program promoted in Britain where participants pledged not to drink during the month of January, and optionally stayed in touch via a Facebook group to support each other.
I took up the challenge on January 2nd, thinking it would be a good way to break my nightly drinking habit. Spending more time with Facebook than I ever had, I commiserated with other DJ'ers. We praised each other's successes and encouraged those who fell off the wagon to try again. Some were aiming for more moderation, some for total abstinence. It was like a continuous online AA meeting, but much more cheerful; the words "alcoholic" and "addict" were rarely heard. "Continuous" because it spanned eleven time zones, with members from California to the Persian Gulf.
I also read a book called This Naked Mind recommended by several in the Facebook group, which promised to "eliminate your desire to drink" by reversing the conditioning of your unconscious mind. It sounded like brainwashing, but I was willing to try. In fact there was nothing subtle or subliminal about the book, aside from one literary ploy that became obvious after awhile. The author fairly beat you over the head with her message.
Between the DJ discussions and my reading, my desire to drink seemed to evaporate. I began to feel better. My moods were lighter, I had more energy and got more done. I took more interest in mundane, daily tasks; they no longer seemed like drudgery. The experience was not new; I'd noticed similar effects in the past when I quit drinking for a few days. I was almost euphoric about these changes during the first weeks, but the novelty wore off.
I completed Dry January and plan to stay dry for good. It hasn't helped the mojo hand, but does eliminate another risk factor for stroke and promotes general brain health. It should help me to better face that ultimate risk factor, for stroke and everything else: age.
Comments
Post a comment...
All comments are moderated. I may answer flame mail directly, but will not post it unless it makes a good point.
References
Revisions to this post:
Funding a Miracle
The Shale Revolution and Related Wonders
Two weeks ago, my wife Kae received a check in the mail for the residual "fair value" of a major investment. Ten years ago, she had bought a limited partnership in a new company drilling for natural gas in one of new shale plays, using the much-hyped fracking technology.
The partnership was bankrupt and was now being liquidated. It had yielded a big tax writeoff in the purchase year and great distributions for two years, but then the annual returns dropped below five per cent and continued to decline (graph below.) She had invested $90,000; the remaining value was about $1500.
It was as if Kae had made a no-interest loan of $90,000, and the borrower defaulted after paying back $54,000- a net loss of $36,000. This was no default, of course; it was all legal- just a risk she took when buying a limited partnership.
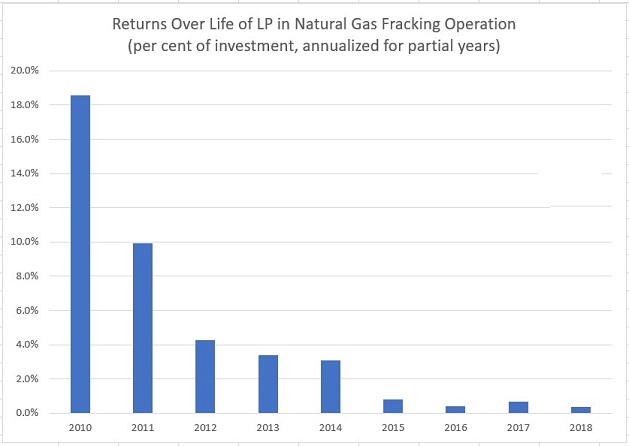
The graph of returns on her investment has the same shape as depletion graphs for fracked shale gas or oil wells. It's not surprising that the returns from an extraction operation should tail off at a rate similar to a well's depletion.
Which was what I feared after the first couple of years, as I learned more about fracking. We had invested in the energy sector for years and made good profits. Given the constant need for energy in every human activity, it seemed like the most secure sector for long term investment. But that was before the fracking miracle.
Our investment advisor had looked at dozens of possible energy investments, including a number of fracking operations. This company seemed to be the soundest of all. Natural gas was cheap at the time, but they had bought hedges on the price which made up for their temporary (we hoped) shortfall.
Three years on, as the returns dwindled, our advisor set up a phone conference with one of the principals. He emphasized how much of Kae's original investment had already been paid back; they always reported this figure with their monthly, later quarterly, distributions. I asked how fast their wells were depleting, and was told I didn't understand the meaning of "depletion." That meant capping wells, shutting down, he said - no depletion here! I asked one or two other questions which he did not answer.
I don't know if the man was consciously obfuscating. He may have had a sort of prospector mentality: his mission in life was to find backers, drill wells and produce gas or oil. Little items like "return on investment" were just numbers for the accountant to play with.
This would have been a good time for Kae to sell out, but she could only sell her interest back to the management, and they weren't buying. It wasn't a good time to sell, they cautioned- always looking out for her interest. Wait for a better time, when they would offer buybacks.
As I learned about the environmental hazards of fracking- the secret chemical mixtures injected, the immunity from EPA regulation- our advisor queried the management about their operations. Very clean and safe, he was told. In fact, their operation was so clean, they contracted to provide safety/environmental training for other fracking firms. Much later in the game, he learned that hydrochloric acid was a major component of fracking fluids.
Kae's loss is not unusual in the energy investment world. It's a commonplace that the shale fracking industry as a whole has never made money, even when oil prices spiked over $100 a barrel. During 2007-2017, though some companies made money in some years, shale operators as a group spent $280 billion more than they earned. Those losses represent bankruptcies, defaults and added debt.
"..shale has been a lousy bet for most investors," according to a 2017 Wall Street Journal article. Since 2007, an index of U.S. producers had fallen by 31%.
When oil prices dropped suddenly in 2014, more than 100 shale producers went bankrupt, defaulting on $70 billion in debt. During 2015-2016, over 1,000 U.S. oil and gas companies (shale drillers and others) filed for bankruptcy.
The shale industry as a whole may show a profit in 2018- the first year ever. And none too soon, because the industry is carrying close to a trillion dollars in debt, half of which will mature by the end of 2019.
A prime example is Anadarko Petroleum, which lost $456 million in 2017. If it had not paid $932 million in interest on its debt, it would have made a half billion in profit. If a company can't afford the interest on its outstanding debt, what happens when the principal comes due?
We won't be investing in limited partnerships again, nor in anything related to shale plays or fracking. As everyone lauds the fracking "miracle", I hope they remember the financial miracles that made it possible- funded by the life savings of thousands like Kae.
Comments
Post a comment...
All comments are moderated. I may answer flame mail directly, but will not post it unless it makes a good point.
References
America's Shale Firms Don't Give a Frack About Financial Returns
The Economist
Wall Street's Fracking Frenzy Runs Dry as Profits Fail to Materialize
Wall Street Journal
IS Fracking Industry in Trouble; Investors Losing Faith
SRS Rocco Report
Top US Shale Producers Exploding Debt Guts Profits
SRS Rocco Report
Higher Prices to Help Oil Companies Refinance
OilPrice.com
Profitability is Finally Within Reach for US Shale
OilPrice.com
Investment Analysis: The Journey of US Light Tight Oil Production Towards a Financially Sustainable Business
International Energy Agency
Energy Secto Bankruptcies: A review of bankruptcy activity in the energy sector: 2015-2016
BankruptcyData, New Generation Research, Inc.
Revisions to this post:
Previous Post:
The Unwanted
Home